
Introduction
Chronic low-intake fluid deficits are endemic in long-term care settings due to:
- Physiological changes of aging
- Comorbidities
- Cognitive and functional impairments
- Polypharmacy
- Environmental factors such as staffing levels
This can result in often preventable primary consequences (acute dehydration) but also secondary consequences and morbidities such as:
- Mood changes
- Impaired psychomotor skills
- Decreased vigor and alertness
- Increased fatigue, headache, musculoskeletal complaints, and reduced care participation (which decreases food and water intake)
- Falls and infection risk
- Delayed wound healing, frailty, and skin health
Low-intake deficits can accumulate over time in a process we call the "dehydration cascade" — where chronic mild low-intake fluid deficits cause clinical consequences on the path to acute dehydration. Recent evidence-based reviews have identified clinical findings associated with the physiology of the cascade, a chain reaction that occurs as the body accumulates a water deficit over time, leading to progressively more severe symptoms and complications ending in acute dehydration.
Crucially, a Cochrane review of evidence strongly emphasizes that best practices for assessing hydration status should not rely solely on laboratory values but rather on clinical findings.
Understanding the basic science of these phenomena can rapidly transform into clinical practices that improve quality of health and outcomes for residents in long-term care.
Hypohydration As a Clinical Entity
Even mild daily deficits over time can initiate the cascade; an average deficit of just 1 ounce/day over 30 days can result in a 2% deficit in a 70kg individual. Hypohydration is a sub-acute state commonly associated with chronic low-intake deficit (1-2%); the hypohydration deficit is insufficient to cause changes in laboratory values but sufficient to produce symptoms. These symptoms result from physiologic phenomena where mild increases in vascular osmotic load drive fluid shifts from intracellular to vascular compartments to maintain homeostasis, causing cellular dysfunction. This normalizing shift in vascular osmolarity prevents thirst triggers and ADH release, creating additional challenges for efforts to improve oral intake.
Clinical consequences of chronic hypohydration include:
- Cognitive and mood impairments
- Musculoskeletal performance
- Headaches
- Increased falls risk
- Delayed wound healing
- Urinary tract infections
- Constipation
Hypohydration also increases the risk of moving down the cascade to acute dehydration; it's a lot easier/faster to go from 2% to 4% deficit than to go from 0% to 4% deficit. This can be triggered by infection (e.g. URI; UTI), reduced participation in care, fatigue, headache or mood changes.
Denying clinically appropriate, RAI-supported hydration does not protect the health system—it increases costs and risk,
Lev added.
Stopping the Cascade
Attempts to "push oral fluids" often fail to stop the cascade, as some form of hyper-hydration is required to overcome the total body deficit.
Typically, such efforts can stall the cascade but create a hypohydration plateau. Acute dehydration is delayed — but the risk remains, and secondary consequences of hypohydration (outlined in the Introduction) persist.
The CMS RAI Manual supports the use of IV fluids "if needed to prevent dehydration if the additional fluid intake is specifically needed for nutrition and/or hydration" when clinically indicated and properly documented.
Intravenous hydration to prevent dehydration is not about returning to hydration baseline (as is the model for treatment of acute dehydration), but over-hydrating via fluid bolus, shifting water back into the cells that have taken the brunt of the compensatory adjustment. The balance of the fluid is naturally excreted once the patient is rehydrated.
Managing Hypohydration in Long Term Care
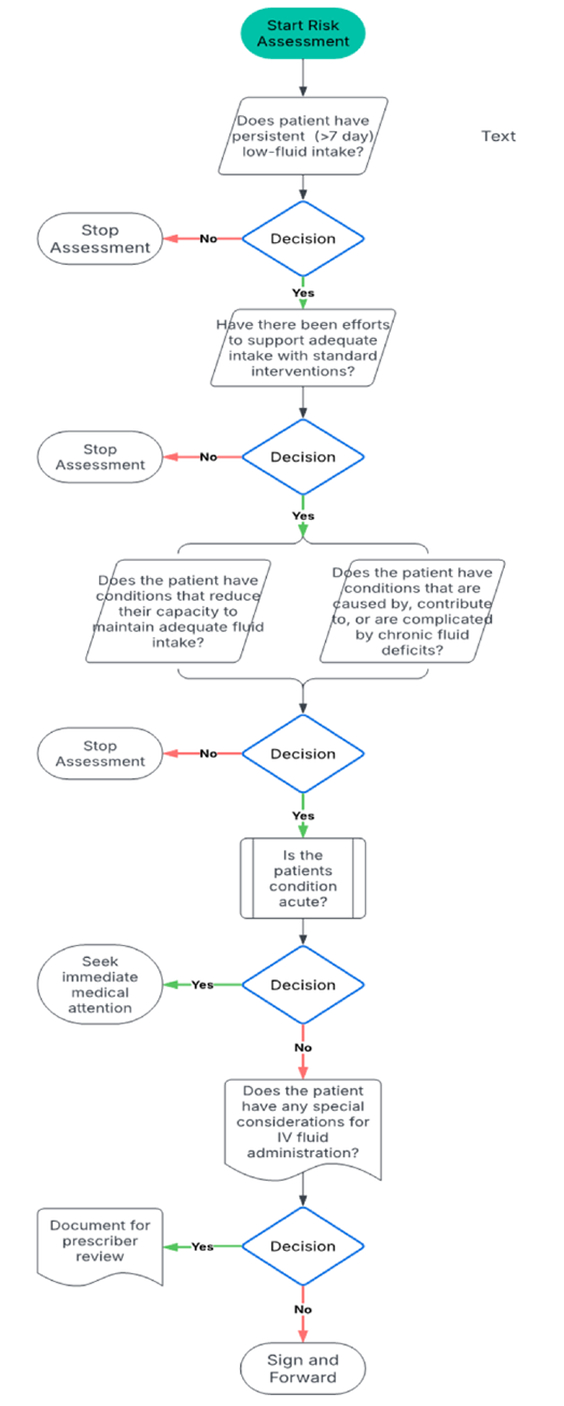
As per the RAI, identifying patients for whom preventive intravenous intervention is clinically indicated requires attentive evaluation and monitoring, progressive intervention including sustained less-invasive interventions, and detailed documentation of medical necessity/rationale.
An algorithm derived from CMS guidance is grounded in four key findings:
- The patient has a chronic low-fluid intake despite efforts undertaken to support adequate fluid intake, and
- The patient has documented conditions and/or medications that interfere with or predispose to limitations in maintaining normal fluid balance, and/or
- The patient has documented conditions known to be caused by, contributed to or complicated by dehydration, and
- The patient has no special considerations or risks associated with intravenous hydration
Managing Hypohydration in Long Term Care (Cont.)
The process of incorporating the provision of preventive intravenous fluids in long-term care has some distinctive operating principles.
First, since the patients are non-acute, they can be identified and scheduled for intervention by cadence (e.g. bi-weekly; monthly).
Second, while any single infusion is likely to reduce risk of acute dehydration, many patients continue to have sustained low-intake post-infusion. This may not support complete resolution of some hypohydration-associated clinical consequences (e.g. mood, ADLs, wound healing) and continued patient monitoring is required to determine whether repeated infusions by cadence may be medically necessary.
Finally, hydration status and nutritional status share many of the same risk factors and chronic low-fluid intake is also associated with micronutrient losses; as the RAI supports preventive intravenous hydration as specifically needed for nutrition and/or hydration, patients may benefit from optional micronutrient supplementation as part of their preventive intervention.

Summary
Dehydration is one of the most preventable causes of avoidable hospitalizations among nursing home residents. Yet, too often, facilities are left reacting to acute collapses rather than proactively preventing them.
The Centers for Medicare & Medicaid Services (CMS), through the RAI Manual acknowledges the clinical place for IV hydration when deployed in a preventative manner. This is not experimental care — it is part of an established regulatory framework for care. Preventive intervention of residents who meet the hypohydration profile can prevent avoidable hydration-related hospitalizations and improve their overall quality of health.
IV hydration for hypo-hydrated SNF residents is more than a clinical intervention — it's a regulatory safeguard, a quality improvement tool, and a QAPI best practice. It directly reduces audit risk, improves publicly reported outcomes, and provides a defensible framework for survey and payer oversight.
Preventative IV hydration is:
Patient-centered:
- Rooted in CMS guidance, the RAI Manual, and Care Area Assessments to reduce the risk of dehydration and hypohydration-associated clinical complications, improve patients' quality of health and avoid preventable hospital transfers
Cost-effective:
- Reduces hospitalizations and ED visits, aligning with both quality and financial stewardship.
Transparent and auditable:
- Supported by facility policies and protocols that ensure appropriate use and reinforce medically necessary interventions.
Compliance-based:
- Integrating hydration management into QAPI brings nursing, dietary, therapy, and medical staff together, showing surveyors a culture of continuous improvement.
- The addition of hypo-hydration monitoring can add insight and needed perspective to many hard-to-address outcomes concerns
Preventive IV hydration is an ideal focus for Performance Improvement Projects (PIP); a focused PIP on hydration can incorporate proactive IV therapy as an evidence-based intervention, documenting patient-centered outcomes and demonstrating clinical compliance to surveyors.
References
- Adan, A. Cognitive Performance and Dehydration. J. Am. Coll. Nutr. 31, 71-78 (2012).
- Barnes, K. & Baker, L. Hydration and team sport cognitive function, technical skill and physical performance. 210, 1-5.
- Barrett KE, Barman SM, Boitano S, Brooks HL. Ganong's Review of Medical Physiology. 26th ed. McGraw Hill; 2019.
- Beck AM, Seemer J, Knudsen AW, Munk T. Narrative Review of Low-Intake Dehydration in Older Adults. Nutrients. 2021;13(9):3142. doi:10.3390/nu13093142.
- Begg DP. Disturbances of Thirst and Fluid Balance Associated With Aging. Physiology & Behavior. 2017;178:28-34. doi:10.1016/j.physbeh.2017.03.003.
- Bhave, G. & Neilson, E. G. Body Fluid Dynamics: Back to the Future. J. Am. Soc. Nephrol. 22, 2166-2181 (2011).
- Centers for Medicare and Medicaid Services Long-Term Care Facility Resident Assessment Instrument 3.0User's Manual. Preprint at https://ltc.health.mo.gov/archives/16022.
- Centers for Medicare and Medicaid Services. Hydration Critical Element Pathway. (2017).
- Edmonds CJ, Foglia E, Booth P, Fu CHY, Gardner M. Dehydration in Older People: A Systematic Review of the Effects of Dehydration on Health Outcomes, Healthcare Costs and Cognitive Performance. Archives of Gerontology and Geriatrics. 2021 Jul-Aug 95:104380. doi:10.1016/j.archger.2021.104380.
- Ferry M. Strategies for Ensuring Good Hydration in the Elderly. Nutrition Reviews. 2005;63(6 Pt 2):S22-9. doi:10.1111/j.1753-4887.2005.tb00151.x.
- Frith J. New Horizons in the Diagnosis and Management of Dehydration. Age and Ageing. 2023;52(10):afad193. doi:10.1093/ageing/afad193.
- Gana, W. et al. Analysis of the Impact of Selected Vitamins Deficiencies on the Risk of Disability in Older People. Nutrients 13, 3163 (2021).
- Hoen L, Pfeffer D, Schmidt JR, et al. Hydration Status of Geriatric Patients Is Associated With Changes in Plasma Proteome, Especially in Proteins Involved in Coagulation. Nutrients. 2023;15(17):3789. doi:10.3390/nu15173789
- Hooper L, Abdelhamid A, Attreed NJ, et al. Clinical Symptoms, Signs and Tests for Identification of Impending and Current Water-Loss Dehydration in Older People. The Cochrane Database of Systematic Reviews. 2015;(4):CD009647. doi:10.1002/14651858.CD009647.pub2.
- Hooper L, Bunn D, Jimoh FO, Fairweather-Tait SJ. Water-Loss Dehydration and Aging. Mechanisms of Ageing and Development. 2014 Mar-Apr;136-137:50-8. doi:10.1016/j.mad.2013.11.009.
- Hooper L, Bunn DK, Abdelhamid A, et al. Water-Loss (Intracellular) Dehydration Assessed Using Urinary Tests: How Well Do They Work? Diagnostic Accuracy in Older People. The American Journal of Clinical Nutrition. 2016;104(1):121-31. doi:10.3945/ajcn.115.119925.
- Hooper L, Bunn DK, Downing A, et al. Which Frail Older People Are Dehydrated? The UK DRIE Study. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2016;71(10):1341-7. doi:10.1093/gerona/glv205.
- Kim, S. Preventable Hospitalizations of Dehydration: Implications of Inadequate Primary Health Care in the United States. Ann. Epidemiology 17, 736 (2007).
- Koch CA, Fulop T. Clinical Aspects of Changes in Water and Sodium Homeostasis in the Elderly. Reviews in Endocrine & Metabolic Disorders. 2017;18(1):49-66. doi:10.1007/s11154-017-9420-5.
- Lacey, J. et al. A multidisciplinary consensus on dehydration: definitions, diagnostic methods and clinical implications. Ann. Med. 51, 232-251 (2019).
- Laur, C. V., McNicholl, T., Valaitis, R. & Keller, H. H. Malnutrition or frailty? Overlap and evidence gaps in the diagnosis and treatment of frailty and malnutritionl. Appl. Physiol., Nutr., Metab. 42, 449-458 (2017).
- Li S, Xiao X, Zhang X. Hydration Status in Older Adults: Current Knowledge and Future Challenges. Nutrients. 2023;15(11):2609. doi:10.3390/nu15112609.
- Marra, M. V. et al. Elevated Serum Osmolality and Total Water Deficit Indicate Impaired Hydration Status in Residents of Long-Term Care Facilities Regardless of Low or High Body Mass Index. J. Acad. Nutr. Diet. 116, 828-836.e2 (2016).
- Maughan RJ. Impact of Mild Dehydration on Wellness and on Exercise Performance. European Journal of Clinical Nutrition. 2003;57 Suppl 2:519-23. doi:10.1038/sj.ejcn.1601897.
- Moy, E., Chang, E., Barrett, M. & (CDC). Potentially preventable hospitalizations- United States, 2001-2009. 62, 139-143.
- Namasivayam-MacDonald, A. M. et al. Inadequate fluid intake in long term care residents: prevalence and determinants. Geriatr. Nurs. 39, 330-335 (2018).
- Nuccio, R. P., Barnes, K. A., Carter, J. M. & Baker, L. B. Fluid Balance in Team Sport Athletes and the Effect of Hypohydration on Cognitive, Technical, and Physical Performance. Sports Med. 47, 1951-1982 (2017).
- Parkinson E, Hooper L, Fynn J, et al. Low-Intake Dehydration Prevalence in Non-Hospitalised Older Adults: Systematic Review and Meta-Analysis. Clinical Nutrition (Edinburgh, Scotland). 2023 42(8):1510-1520. doi:10.1016/j.clnu.2023.06.010.
- Pence J, Davis A, Allen-Gregory E, Bloomer RJ. Hydration Strategies in Older Adults. Nutrients. 2025;17(14):2256. doi:10.3390/nu17142256.
- Pershad, J. A systematic data review of the cost of rehydration therapy. 8, 203-214.
- Porter, K., Hoey, L., Hughes, C. F., Ward, M. & McNulty, H. Causes, Consequences and Public Health Implications of Low B-Vitamin Status in Ageing. Nutrients 8, 725 (2016).
- Riebl, S. K. & Davy, B. M. The Hydration Equation. ACSMs Heal. Fit. J. 17, 21-28 (2013).
- Schols JM, De Groot CP, van der Cammen TJ, Olde Rikkert MG. Preventing and Treating Dehydration in the Elderly During Periods of Illness and Warm Weather. The Journal of Nutrition, Health & Aging. 2009;13(2):150-7. doi:10.1007/s12603-009-0023-z.
- Services, C. for M. & M. LTC Surveyor Guidance 2024 (QSO-25-07-NH). (2021).
- Smith, M. F., Newell, A. J. & Baker, M. R. Effect of acute mild dehydration on cognitive-motor performance in golf. 26, 3075-3080.
- Stookey, J. D. High Prevalence of Plasma Hypertonicity among Community-Dwelling Older Adults: Results from NHANES III. Journal of the American Dietetic Association 105, 1231-1239 (2005).
- Tuna, H. İ. Determination of Daily Fluid Intake Levels and Affecting Factors of Elderly Individuals Living at Home. Genel Tıp Derg. 34, 153-157 (2024).
- Wysocki, A. et al. The Association between Long-Term Care Setting and Potentially Preventable Hospitalizations among Older Dual Eligibles. Heal. Serv. Res. 49, 778-797 (2014).
- Xiao, H., Barber, J. & Campbell, E. S. Economic burden of dehydration among hospitalized elderly patients. Am. J. Heal.-Syst. Pharm. 61, 2534-2540 (2004).



